
By David Dardashti Topic: Neuro-Pharmacology
Mental Health Innovation
Read Time: 10 Minutes
The current landscape of depression treatment is characterized by a tragic lack of precision. For decades, psychiatry has relied on a “throw everything at the wall and see what sticks” approach—cycling patients through SSRIs, SNRIs, and talk therapies with widely variable results. When dealing with Treatment-Resistant Depression (TRD), this trial-and-error method is not just inefficient; it is devastating to the human spirit.
Depression is not a single biological error; it is a complex architecture of trauma, biology, and entrenched psychological defense mechanisms. To treat it effectively, we must move beyond standard protocols and embrace algorithmic precision.
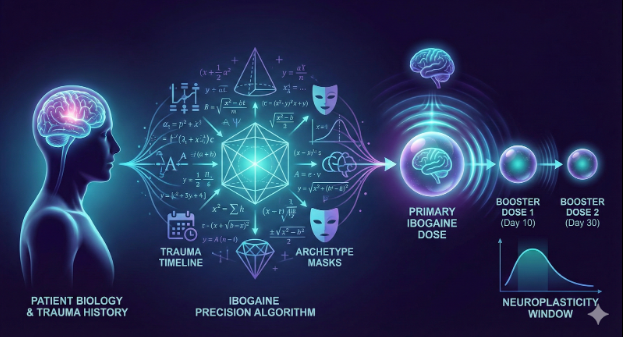
At our facility, we have developed a pioneering algorithmic approach to Ibogaine treatment for depression. Ibogaine is unique among psychedelics for its ability to induce a profound “life review” alongside a neurobiological reset. However, its power demands accuracy. By integrating biological metrics, trauma timelines, and advanced mathematical concepts related to psychological archetypes, our algorithm calculates a treatment path as unique as the individual’s own neural fingerprint.
Here is a look inside the mathematics of healing the modern mind.
Phase 1: The Biological Baseline – Safety and Security
Before we can address the psyche, we must secure the biology. Depression takes a physical toll on the body, and Ibogaine is a metabolically demanding substance. The foundation of our algorithm is a rigorous computation of physical safety constraints.
We do not simply glance at a medical chart. We input hard data points—age, weight, height, and general cardiovascular health—into our model. This allows us to calculate the patient’s Metabolic Load Capacity.
A 25-year-old athlete and a 55-year-old with hypertension may have the same level of depression, but their physiological ability to process Ibogaine is vastly different. The algorithm analyzes liver enzyme activity (specifically CYP2D6) alongside cardiac metrics to determine the maximum safe saturation point. This ensures the treatment remains a controlled medical procedure rather than a physiological gamble, providing the security necessary for the patient to surrender to the psychological experience.
Phase 2: Quantifying the Intangible – The Trauma Timeline
Once safety is established, the algorithm turns to the core driver of depression: unprocessed trauma. But how do you quantify trauma?
Our protocol treats trauma not as a story, but as a data set with specific variables that influence dosing requirements for successful introspection:
- The Temporal Variable (Time Elapsed): A trauma that occurred 30 years ago has had decades to engrain itself into the patient’s neural pathways and personality structure. It has become structural. Recent trauma is often more acute but less neurologically entrenched. The algorithm adjusts the dosing velocity based on how “deeply buried” the root cause is.
- The Developmental Variable (Age at Occurrence): Trauma experienced during critical childhood developmental windows impacts brain architecture differently than adult trauma. The algorithm accounts for these developmental interruptions, often necessitating a different therapeutic approach to unlock those early-stage memories.
- The Typology Variable: We differentiate between acute shock trauma (e.g., a car accident) and complex, relational trauma (e.g., long-term narcissistic abuse). Complex trauma often requires a cumulative dosing strategy rather than a single “flood,” allowing the patient to peel back layers slowly without psychological destabilization.
Phase 3: Abstract Algebra and the Geometry of Archetypes
Perhaps the most innovative aspect of our algorithmic approach is how we handle the psychological defenses a patient uses to survive.
Over time, people with treatment-resistant depression develop sophisticated coping mechanisms. In Jungian psychology, these can be viewed as “personifications” or archetypes—structural roles the ego plays to avoid pain (e.g., The Martyr, The Perfectionist, The detached Observer). These are not just habits; they are rigid psychological structures that block healing.
How do you dose for an archetype? We utilize concepts drawn from Abstract Algebra.
In mathematics, abstract algebra deals with algebraic structures—groups, rings, and fields—mapping the relationships between sets rather than just numerical values. Our algorithm conceptualizes a patient’s coping mechanisms as interconnected algebraic structures.
By mapping the relationships and rigidity of these archetypes, the algorithm calculates the precise “force” required to disrupt them. We are essentially calculating the energy needed to temporarily dissolve the ego’s rigid algebraic structure, allowing the patient to step outside their habitual “personifications” and view their trauma from a place of objective clarity. Too little dose, and the archetype defends itself; too much, and the experience becomes chaotic. The algorithm finds the precise window of integration.
Phase 4: The Sustainability Quotient – Cognitive Awareness and Boosters
The initial Ibogaine treatment opens a critical window of neuroplasticity—a period where the brain is malleable and open to change. But the long-term success of treating depression relies on what happens in the weeks that follow.
Our protocol includes a pre- and post-treatment assessment of the patient’s Overall Cognitive Awareness and integrative capacity.
- How readily does the patient connect their behaviors to their emotions?
- What is their capacity for self-reflection independent of the medicine?
Patients with lower baseline cognitive awareness often struggle to integrate the profound insights of the Ibogaine experience once the acute effects wear off. The algorithm tracks this “Awareness Quotient” to determine the necessity and timing of booster doses.
A highly aware patient may only need talk therapy for integration. A patient struggling to hold onto the insights may be scheduled by the algorithm for smaller, sub-psychedelic booster doses at the 10-day and 30-day marks to sustain the neuroplastic window and solidify the new neural pathways against the return of depressive loops.
Conclusion: The Future is Calculated Compassion
Depression is a thief that steals vitality, hope, and the future. For too long, the medical community has fought this sophisticated enemy with blunt instruments.
At our facility, we believe that true compassion in medicine means utilizing the highest level of scientific rigor to relieve suffering. By translating the complexities of biology, trauma history, and psychological archetypes into a cohesive algorithmic framework, we are moving Ibogaine treatment out of the fringes and into the future of precision psychiatry.
We don’t just hope you get better. We calculate the path to your recovery.
For more information visit www.ibogaineclinic.com/ibogaine-treatment

